
Picture a Series A healthtech startup fresh off an $8 million funding round. The board wants rapid user acquisition. The CTO wants to build a proprietary patient management system to handle specialized clinical workflows. The CEO, eager to show momentum, approves the build.
Eight months later, the runway is shrinking. The engineering team is exhausted. The system is half-finished because the team underestimated the complexity of HIPAA-compliant data routing and FHIR standards. To stop the cash burn, they scrap the custom build and buy a white-labeled off-the-shelf solution. They lost nearly a year of development time, burned hundreds of thousands of dollars, and now have to justify a massive pivot to their board.
I’ve seen this scenario play out more than once. A founder comes to us six months after a build decision that made sense on paper — and we spend the first discovery call understanding what went wrong rather than what to build next.
You hold the final authority on budget and vendor selection, even if you delegate technical evaluation to your CTO. Every build vs buy decision directly impacts your runway, your regulatory risk, and your ability to scale. The wrong call doesn’t just slow you down — it can end the company.
Why doesn’t the standard build vs buy logic apply in healthcare?
In standard B2B SaaS, the rule is straightforward: build what makes you unique, buy the commodities. Need a CRM? Buy it. Need a proprietary recommendation algorithm? Build it.
Healthcare breaks this logic in three specific ways.
Compliance is structural, not optional. Whether you operate under HIPAA in the US or equivalent frameworks in other markets, every system that touches patient data must handle it with strict security controls baked into the architecture — not patched in later. When you buy an off-the-shelf tool, you’re inheriting their compliance posture. If they fail an audit, you fail an audit.
Interoperability is non-negotiable. Your system rarely exists in isolation. It must connect to EHR systems, lab platforms, billing clearinghouses, and insurance APIs. Standard software is built around clean, predictable APIs. Healthcare runs on complex legacy standards like HL7 and evolving frameworks like FHIR. Tools that claim easy integration almost always require heavy customization to work in a real clinical environment.
Clinical workflows don’t map to generic product categories. A scheduling tool built for a hair salon will not work for a multi-specialty clinic that needs to verify insurance eligibility, track clinical prerequisites, and manage overlapping provider schedules. Off-the-shelf solutions often force clinicians into rigid workflows — and low clinical adoption is one of the fastest ways to lose a hospital contract.
When does buying make more sense than building?
Protecting your runway means knowing when to write checks instead of code. Buying makes clear business sense in these specific situations.
Core infrastructure and security. Never build your own secure cloud hosting, database management, or identity verification systems. AWS, Google Cloud, and specialized healthcare infrastructure providers have already solved these problems at scale. Buying these services gives you compliance peace of mind immediately and keeps your engineering team focused on your actual product.
Standardized communication. If your platform needs telehealth video, secure messaging, or SMS notifications, buy the underlying technology. Specialized healthcare communication APIs offer compliant solutions that would take months to replicate. Rebuilding a secure video streaming protocol adds zero competitive advantage.
Established EHR integrations. Avoid building custom point-to-point connections with Epic, Cerner, or Athenahealth where aggregator platforms already exist. Integration engines that translate and route this data reduce your technical overhead and speed up deployment — which means faster traction to show investors.
Back-office operations. Billing, HR, and internal team communication should run on established enterprise software. Your competitive advantage doesn’t live in how you process payroll.
When does custom healthcare software development make the right call?
Buying saves time on commodities. Building protects your valuation. Your Series A or B funding needs to be justified by owning the technology that drives your business model. These are the triggers that indicate you need custom healthcare software development:
- Your core clinical algorithm or IP. If your company’s primary value proposition is a unique diagnostic model, a proprietary care pathway, or an AI-driven triage system, you must build it. Relying on a third-party vendor for your core differentiator leaves you exposed to their pricing changes, feature deprecations, and acquisition by a competitor.
- Highly specific provider workflows. Clinician burnout is a real adoption risk. If off-the-shelf tools force doctors or nurses through five irrelevant screens to complete a simple task, they will abandon your platform. When your success depends on provider adoption, building a custom interface that matches their exact workflow is a necessity, not a luxury.
- Deep patient engagement models. Standard patient portals are built for the average case. If your business model relies on daily patient engagement — chronic care management, behavioral health tracking, remote patient monitoring — a generic tool will produce high churn. Custom development gives you control over the user experience and the ability to integrate specialized tracking that off-the-shelf tools can’t support.
- Complex or proprietary analytics. If your business requires combining clinical, financial, and operational data into proprietary predictive models, standard reporting dashboards will fall short. This is especially true when your analytics layer is part of what you’re selling to hospital systems or payers.
What is the hybrid trap in healthcare software development?
The hybrid trap is the most common mistake I see at Series A. It feels like a compromise. It rarely is.
Many founders try to hedge by purchasing a commercial off-the-shelf platform and customizing it heavily. You buy a platform that covers 60% of your needs. Your CTO builds custom workarounds and middleware to handle the rest. In practice, you’ve created a brittle, expensive ecosystem. Every time the vendor updates their core software, your custom integrations break. Your engineering team spends their cycles maintaining the glue instead of building new features.
A useful rule of thumb: if a tool requires more than 20% customization to fit your business, you’re usually better off building from scratch or finding a different vendor. The hybrid approach often costs more than either option done cleanly — and it leaves you with the worst of both: enterprise subscription fees plus the full engineering payroll burden.
How should you actually compare the cost of building vs buying healthcare software?
Most founders get this calculation wrong. They compare the annual subscription fee of a vendor against the salaries of the engineers needed to build the same thing — and stop there.
The complete comparison is different. When you buy, factor in implementation costs, data migration, staff training, and vendor lock-in risk. If a vendor raises their prices 30% next year, how difficult is it to switch? You also need to monitor their compliance posture continuously — because their audit failure becomes yours.
When you build, the true cost goes well beyond writing the initial code. Software requires ongoing security patches, framework updates, and infrastructure costs. Every sprint your team spends building a patient scheduling module is a sprint they didn’t spend improving your core product. And finding engineers who understand HIPAA compliance, FHIR standards, and healthcare interoperability is both difficult and expensive. The U.S. Health Resources and Services Administration projects continued shortages across key health IT occupations through 2038 — a structural gap that makes hiring specialized clinical software engineers one of the most time-consuming and costly decisions a healthtech founder can make.
In my experience working with healthtech founders on these decisions, the cost gap between custom and off-the-shelf is smaller than most expect — and it’s getting smaller. At Impressit, we built FlowForge specifically to address this: it’s an AI-native delivery system that encodes senior engineering judgment into repeatable workflows, which means complex clinical systems get built faster and with less resource overhead than a traditional custom build. When you factor that into the five-year total cost of ownership, the case for custom becomes even stronger than the subscription math suggests.
The right comparison uses a five-year total cost of ownership — including maintenance burden and the explicit opportunity cost of your engineering resources.
A practical decision framework for build vs buy in healthcare
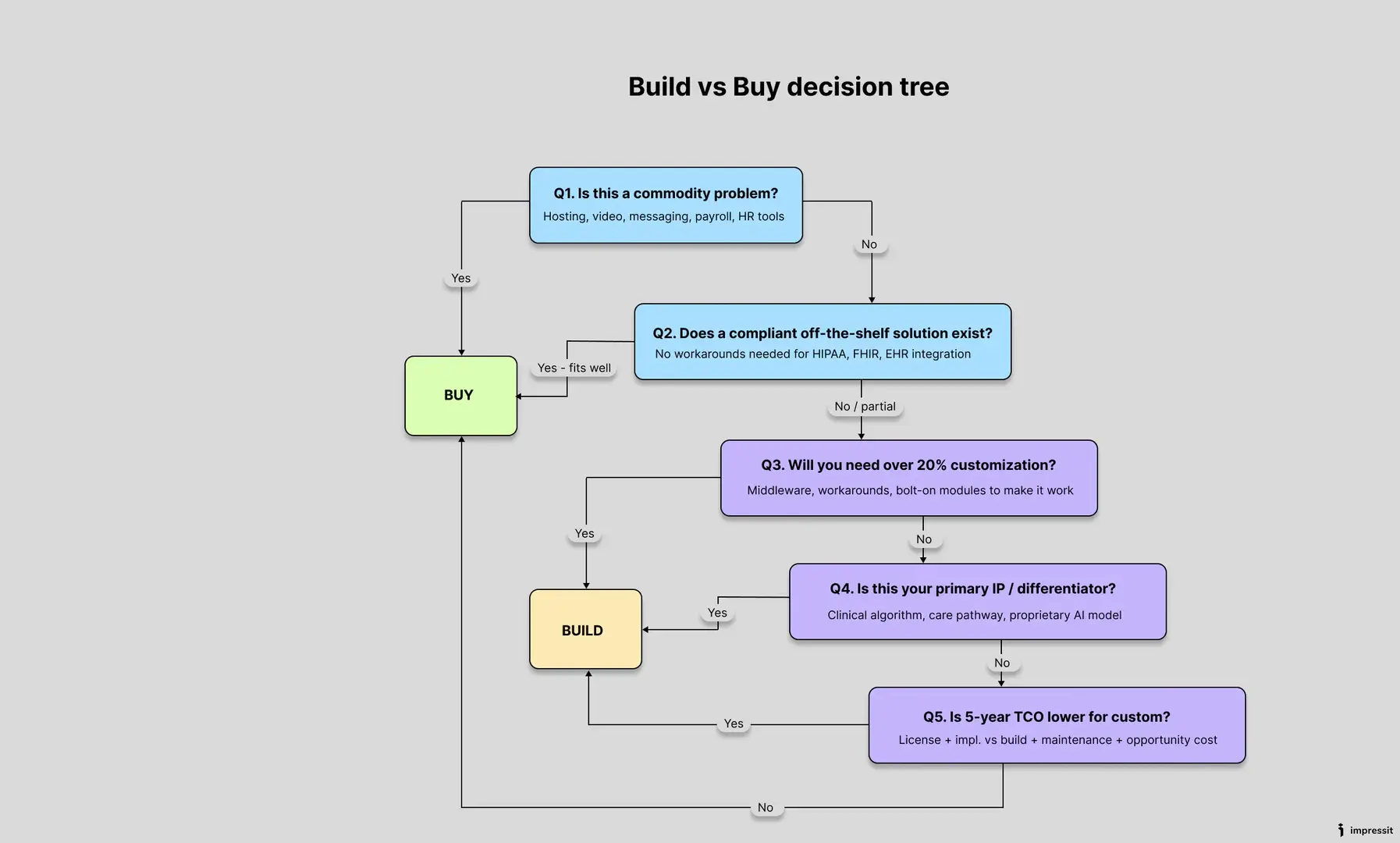
Use these five questions with your CTO before committing to either path.
- Is this a commodity or a core business problem? If it’s a commodity — hosting, video, messaging — buy it.
- Does a compliant off-the-shelf solution exist? If no vendor meets your regulatory requirements without significant workarounds, build.
- Will we need to customize a purchased tool by more than 20%? If yes, avoid the hybrid trap. Build it yourself.
- Is this our primary intellectual property? If the feature is the main reason investors funded you, build it and own it completely.
- What is the five-year total cost of ownership? Calculate vendor subscription costs plus implementation costs versus initial development costs plus ongoing maintenance. Choose the path that protects your runway best.
Closing thoughts
The build vs buy decision in healthcare is rarely a one-time event. Systems you bought in year one may need to be replaced by custom builds in year three. Custom features you built early on might be better replaced by newly available enterprise tools as the market matures.
The founders who navigate this well treat technology decisions as business decisions. They build where the problem is clinically specific and competitively differentiated. They buy everything else — and they revisit the decision as the company scales.
Look at your current product roadmap. Which upcoming feature is consuming the most engineering time for the least competitive return?
–
Roman Zomko is Co-Founder and CEO of Impressit, a software development company specializing in custom healthcare software development, AI integration, and dedicated engineering teams for regulated industries. Impressit has worked with healthtech companies across the US and UK, including Carbon Health and HCSG, on projects ranging from clinical infrastructure to remote patient monitoring systems. Impressit’s AI-native delivery system FlowForge enables faster and more cost-efficient delivery of complex custom software compared to traditional development approaches.
Editor’s Note: The opinions expressed here by the authors are their own, not those of Impakter.com — In the Cover Photo: How to choose a Healthcare Software. Cover Photo Credit: Freepik





